Nociceptors are pain sensors that report actual or threatened tissue damage as a pain stimulus to the brain for further processing. Three groups of Nociceptors are able to differentiate between mechanical, thermal and chemical overloads. Nociceptors are distributed throughout tissue, except in the mesenchyme of the brain, lungs and liver, a particular cluster is found in the skin.
What are nociceptors?
Nociceptors are sensory nerve endings that belong to the class of mechanoreceptors and are found in all tissues of the body except in the mesenchyme of the liver, lungs and brain, the specialized functional tissue of the organs. A particular concentration of nociceptors can be found in the skin. Unlike the other mechanoreceptors, the nerve endings of the nociceptors do not have special sensor heads, but are so-called free nerve endings that branch out towards the periphery.
Three different groups of nociceptors allow a differentiation of pain perception between mechanically, thermally or chemically triggered actual or threatening injuries. Depending on the type and location of the nociceptors, pain stimuli can be localized well or less well. The dense distribution of nociceptors in the skin usually allows for good localization, while nociceptors located far inside in the muscles, on the bones and in the connective tissue usually only trigger a dull, not precisely localizable pain sensation.
It is the so-called deep pain, while the easily localizable pain in the skin is also referred to as surface pain. In addition, nociceptors in the intestines can trigger visceral pain, which is also difficult to localize and which can sometimes be very severe, such as in renal colic or appendicitis.
Anatomy & structure
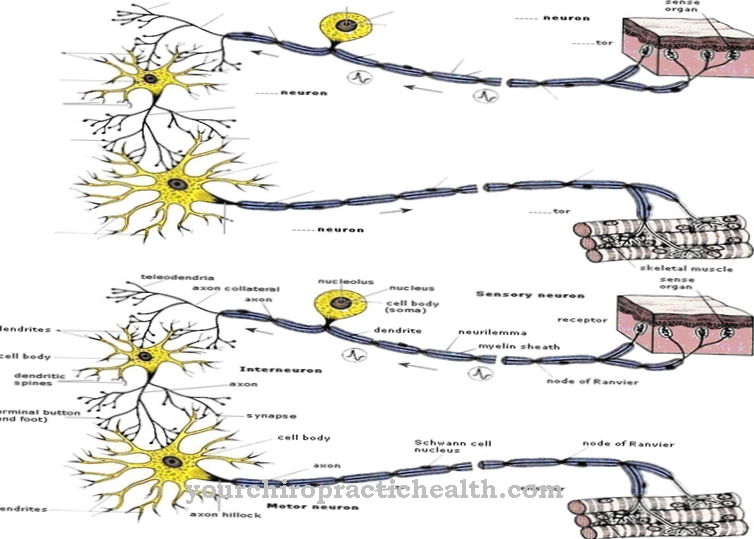
Depending on their function, nociceptors consist of differently structured afferent nerve fibers that differ in their stimulus generation and stimulus transmission behavior. A group of mechano-nociceptors that react to strong mechanical stimuli such as pressure, impact, stabbing and pulling as well as twisting, fall under the category A-Delta fibers with a diameter of 3 - 5 µm and are surrounded by a thin myelin layer. Your stimulus transmission speed is 15 m / sec.
Weaker mechanical stimuli are picked up by mechanoreceptors of the tactile system, with which the nociceptor system is closely connected via synapses. The group of thermo-nociceptors, which react to temperature stimuli above 45 degrees Celsius and to cold stimuli, usually belong to the C-polymodal afferents, which also react to strong mechanical and chemical stimuli. The nerve fibers are extremely thin at 0.1 to 1 µm, have no medullary sheath and are characterized by a slow transmission speed of around 1 m / sec, which is unsuitable for generating protective reflexes. C-fibers also predominate in visceral nociceptors, which are responsible for producing dull, dragging deep pain.
Characteristic of nociceptors of all categories are their free branched nerve endings, which do not have specialized sensor heads. Substances that excite nociceptors are called algogens. Known algogens are neurotransmitters such as serotonin, histamine and bradykinin, a polypeptide that constricts blood vessels.
Function & tasks
Nociception often overlaps with the tactile and haptic sensor system, because both systems must have qualitatively similar sensory capabilities. However, nociception is about avoiding situations that have led to an injury in the future or immediately - if necessary even reflexively - interrupting situations that would lead to an injury if continued.
The main task of the various nociceptors is therefore to report mechanical, thermal or chemical stimuli that have led to an injury to the CNS as pain stimuli and not as quantitative sensory stimuli like the haptic and tactile system. The CNS then summarizes all available information and sets the corresponding pain stimulus. At the same time, the sensory parameters that led to the injury are stored in the pain memory in order to avoid such situations in the future. This means that the nociceptors are sensitized accordingly.
A perceived pain cannot be triggered directly by the nociceptors, but is an expression of a processing process of certain centers in the CNS. There is not only "pain", but other vegetative reactions such as changes in blood pressure and heart rate, changes in intestinal peristalsis, motor reactions such as reflex movements, facial expressions and much more can be triggered simultaneously. Nociceptors protect the body from injury. They take on a warning function when parameters are threatened to be exceeded, which could lead to injuries.
You can find your medication here
➔ Medicines for painDiseases
Problems related to the sensation of pain can affect the nociceptors directly through a lower or higher response threshold or through a general dysfunction. Problems with the further processing of the nociceptive action potentials are more common than a general dysfunction of the nociceptors. It is then no longer the classic nociceptive pain, but neuropathic pain, which is often chronic, i.e. it persists even after the immediate cause of the pain has already been eliminated.
What causes chronic neuropathic pain is not (yet) fully understood. Neuropathic pain can be associated with positive or negative symptoms, which means that in the case of positive symptoms, the stimulus threshold for triggering pain sensation in the form of hyperalgesia is reduced, i.e. pain sensation occurs with minor stimuli. Opposite symptoms are also known, which can lead to a reduced sensation of pain up to a complete insensitivity to pain, the analgesia.
In the well-known diabetic neuropathy, which is caused by damage to the pain-reporting nerves, positive and negative symptoms appear side by side. Fibromyalgia or soft tissue rheumatism is also associated with neuropathic sensory pain disorders. Usually it is a form of hyperalgesia. An example of negative symptoms including analgesia is provided by the mental illness of borderline disorder. Those affected can even cut themselves without feeling pain.